 English
English عربى
عربى Español
EspañolLiterature review UBE surgery "lamina clamp-free" decompression
A common complication of UBE surgery is occasional dural tear. With the accumulation of experience in minimally invasive spinal surgery, the author of the article realized that the laminae clamp is the surgical instrument most likely to cause dural tear or nerve root injury. Therefore, the author proposed the "lamina clamp-free" technique in UBE surgery. It provides good treatment effect, sufficient nerve decompression, excellent facet joint protection and low complication rate.
Surgical technique
Take L4-5 left-sided approach for UBE unilateral approach and bilateral decompression as an example.
(Try not to use laminae clamps during decompression to avoid dural tear).
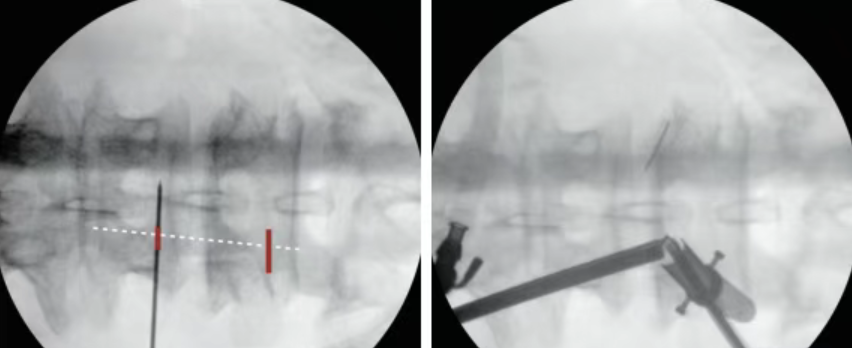
X-ray positioning
The target area is the junction of the spinous process and lamina, and the skin incision is located at the intersection of the medial edge of the left L4 and L5 pedicles and the lower edge of the pedicles. The cephalad skin incision (about 6 mm) is the entrance for the endoscope, and the caudal skin incision (about 10 mm) is the entrance for the instrument.
The endoscope and step-by-step dilation were inserted separately, converged at the junction of the spinous process and lamina, and the position was confirmed by fluoroscopy.
Radiofrequency was used to treat soft tissue and stop bleeding to create a clear surgical field.
Placing a distraction channel at the working entrance can maintain good saline outflow.
Osteotomes with 3 different bending angles: 0°, 10° and 20° were designed for the "lamina-free clamp" decompression technique.
The osteotomy was 4 mm wide, 2 mm thick, and the tip was symmetrically tapered.




Endoscopic decompression
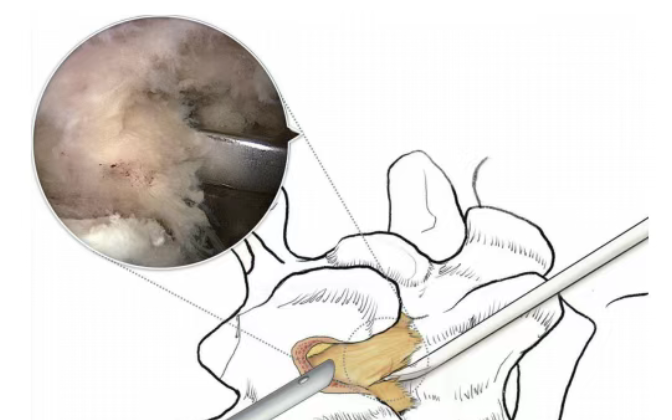
The lamina was removed from the L4 spinous process and lamina junction using a burr.
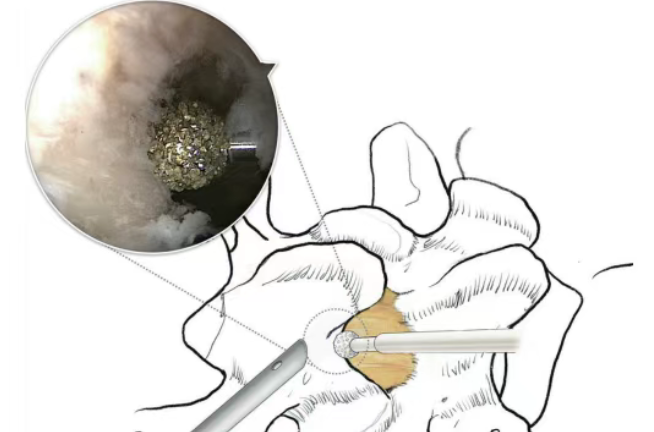
The lamina is removed laterally until the origin and insertion of the caudal ligamentum flavum are exposed and the epidural fat is exposed.

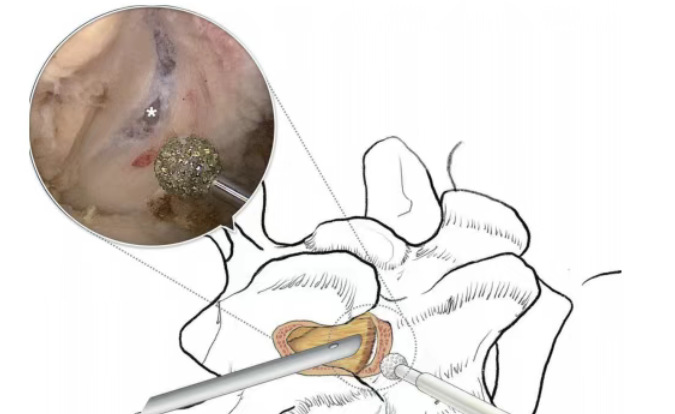
Use a dissector to dissect the L5 lamina head and remove the superficial part of the ligamentum flavum.
Use a burr to work on the head of the L5 lamina and the base of the spinous process until the deep layer of the ligamentum flavum is exposed.
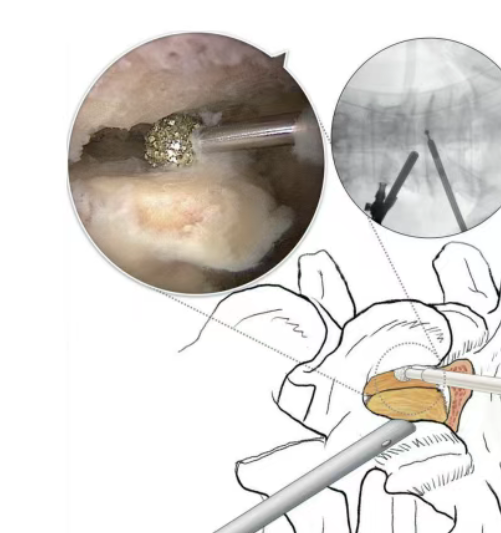
Move the burr along the superior edge of the L5 lamina toward the contralateral side. If possible, resect the superficial portion of the contralateral ligamentum flavum (to provide more working space for contralateral decompression). Identify the inferior edge of the spinous process. Use the dissector to separate the ligamentum flavum from the spinous process of L4 and the contralateral lamina.

The bur is moved to the space between the contralateral lamina and ligamentum flavum for sublaminar decompression. If the ligamentum flavum is still present, the bur can be advanced into the contralateral recess.
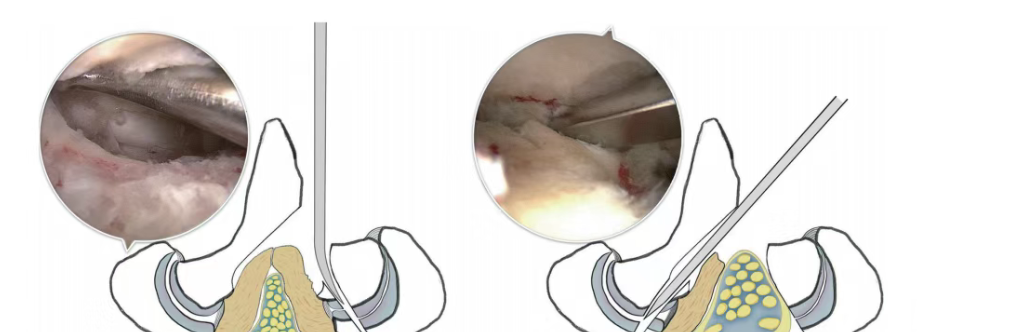
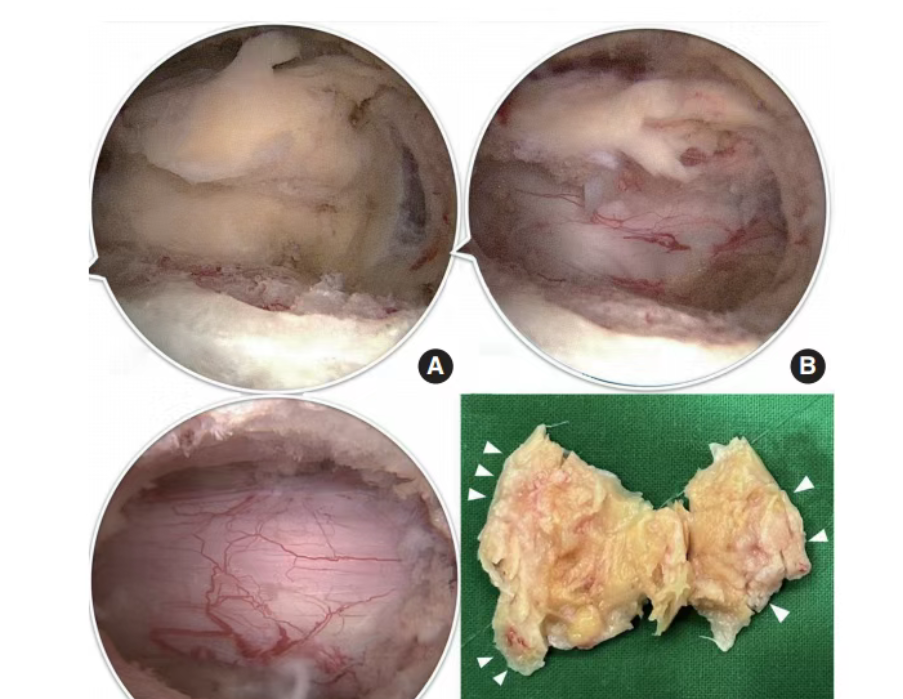
The yellow ligament is kept intact until the bone decompression is completed. The osteotomy tool is used to decompress the ipsilateral lateral recess. On the medial side of the superior articular process of L5 and the inferior articular process of L4, the superior articular process of L5 and the inferior articular process of L4 are removed using the osteotomy tool.

Torque the bone fragments and separate the ipsilateral ligamentum flavum from beneath the L4 inferior articular process and lamina. Use a nucleus pulposus forceps to grasp the bone fragment and remove it as a whole with the ipsilateral ligamentum flavum. The osteotomy tool processes the head of the contralateral L5 lamina. Confirm the contralateral L5 superior articular process along the lamina. Resect the contralateral L5 superior articular process
The bone fragment and the contralateral ligamentum flavum were separated from their attachments. The ligamentum flavum was then grasped with a nucleus pulposus forceps and removed in one piece along with the bone fragment.
Exploration for hemostasis
Explore for residual stenosis. Use radiofrequency hemostasis. Use bone wax for bone surface hemostasis. Temporarily stop saline irrigation to check for any occult bleeding.
22:53:31







")